HIATUS HERNIA REPAIR
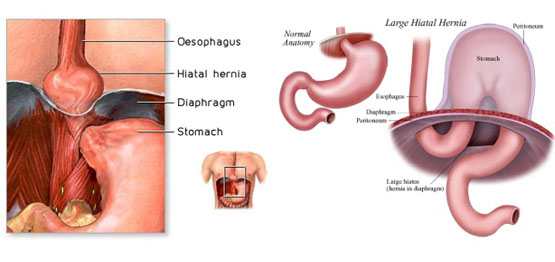
The oesophagus runs through the diaphragm to the stomach and carries food from the mouth to the stomach. The oesophagus passes through the diaphragm just before it meets the stomach, through an opening called the oesophageal hiatus. When the opening (hiatus) in the muscle between the abdomen and chest (diaphragm) is too large, some or all of the stomach (can also include a portion of bowel) can slide up into the chest cavity.
This can cause heartburn (gastro-oesophageal reflux: GORD) as gastric acid backflows from the stomach into the oesophagus, pain and breathlessness especially after eating due to the reduced space in the thoracic cavity.